

Metabolic Disease Related to Obesity
Obesity Dilemma Blog
The sedentary lifestyle and the prompt availability of cheap foods make obesity a significant concern in this modern world. Obesity is not a single problem but gives rise to several issues related to metabolic, inflammatory, and degenerative disorders. The most deadly consequence of obesity is the effect on the cardiovascular system, which leads to atherosclerotic cardiovascular disease (ASCVD). Other than atherosclerotic cardiovascular disease, the risk of many conditions related to kidney, joints, central nervous system, liver, type 2 diabetes, and certain cancers also increases.
Kidney problems:
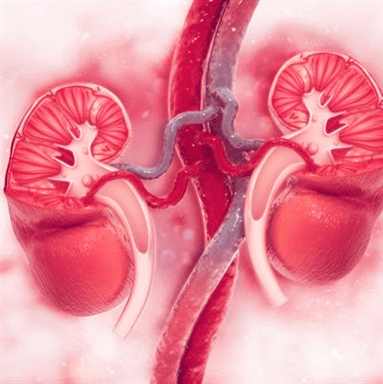
Obesity gives rise to many health problems. One of the alarming problems caused by being overweight is a kidney problem. Obesity can lead to the development of long-term abnormalities in the functioning of the kidneys leading to the condition called chronic kidney disease. People with overweight have high energy demands of the body. Due to this, the metabolic rate of the body increases. The increase in the body’s metabolic rate is followed by the increase in the pressure of fluid in the kidney. The continuous high pressure in the kidney, also known as high intraglomerular pressure, damages the kidney’s structure. When the load on the kidneys exceeds the organ’s capacity, damages occur, which in severe cases can cause life-threatening conditions.(1) The loss of protein in the urine increases among obese people. The loss of essential proteins in the urine also deprives the body of the crucial factors which play an essential role in body functioning and the defense system. Due to the low functioning of the kidney, the urine becomes acidic. The loss of ions like sodium and phosphate also increases, which changes the blood chemistry and compromises bone health. The greater amount of oxalate ions in the urine predisposes the body to risk of kidney stones. In the case of extreme high BMI, the filtration process in the kidney exceeds the safe limit and can lead to complications, including kidney-related cancers. Because in an obese person, the growth factors are also high, which can increase the cell turnover in the already compromised kidney leading to the development of tumor cells.(2) (1)
Joint Problems:
Obesity is a significant risk factor for soft tissues and joint trauma—the whole weight of the body balances on the joints of the body. When the body’s weight increases, the load on the joints also increases. The joints affected mainly by the overweight carry the most weight of the body, like hip and knee joints. The one-kilogram increase in weight causes a four to six-kilogram increase in load on the joints. The sports injuries in obese people are higher than in non-obese people. The obese person is more liable to fractures, ligament tears, and various ankles, knee, and hip joint injuries. The risk of knee displacement increases with the increase in body weight. Obesity is the leading cause of the wear and tear problem of the joints, known as osteoarthritis.(3) The fat cells in the obese person continuously release the inflammatory mediators, which cause inflammation in the joints and cause extreme damage.

The extra weight can cause damage to the cartilage of the joints leading to the condition known as arthritis. Similarly, the risk of damage to the connective tissues also increases, leading to the condition known as tendonitis. In these conditions, the joints become extremely painful and inflamed. (3)
Brain Problems:
It is found that the blood flow to the brain decreases in an overweight person. The decrease in blood flow is caused by the high cholesterol level in the blood, narrowing the arteries supplying the body. The decreased blood flow to the brain compromises the brain’s functioning and leads to various brain problems related to obesity. The overweight person has more risk of depression, bipolar disease, and suicide. The problems related to the memories like dementia and Alzheimer’s disease also increase. A study proved that an obese person has less grey matter and white matter in the brain. The reduction in the matter is associated with decreased brain cognitive function. Overnutrition causes inflammation in the brain. The fat cells also release the inflammatory mediators, which cross the blood-brain barrier and increase the inflammatory process in the neurons known as neuroinflammation. The inflammation causes the degeneration of the neurons called neurodegeneration. The imbalance in the gut microorganisms also damages the cluster of neurons in the gut. As a result, systemic inflammation occurs and leads to severe brain conditions. The inflammation further reduces blood flow to the brain and deprives the brain of oxygen. Cell death occurs and causes irreversible damage to the brain. (4–6)
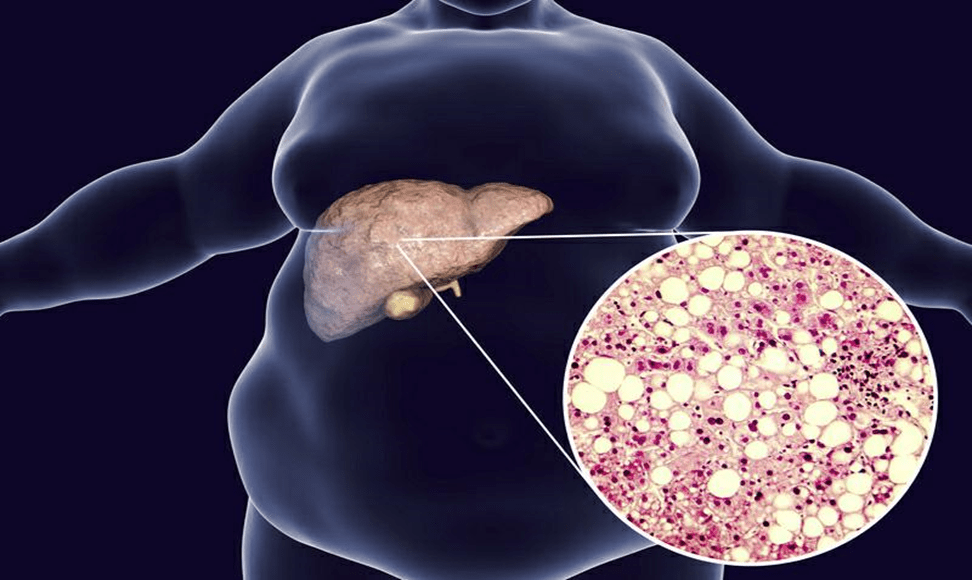
Fatty liver:
The liver is the body’s primary organ with a dual blood supply. The fats in the body break down to produce free fatty acids in the blood. The liver uptakes the fatty acids, and the metabolism of fatty acids occurs in the liver. In the case of overweight, the demand of the body increases. Fat cells release an extra amount of fatty acids. The fat cells release non-esterified free fatty acids, which disrupt the composition of the blood. The liver’s rate of fatty acid uptake exceeds the liver’s capacity for fatty acid metabolism. Due to this, the level of triglycerides in the liver increases, leading to a condition known as nonalcoholic fatty liver disease (NAFLD). The greater
Diabetes:
Obesity is the major risk factor for the development of diabetes. In an obese person, the circulating sugar level is higher than that of a non-obese person. The continuous high sugar level triggers the insulin from the pancreas. The continuous triggering of the pancreatic cells increases the organ’s cells in response to more demand. Ultimately, the cells die when the load on the pancreas exceeds the organs’ limit. This leads to the development of type I diabetes in an obese person—also, the risk of type II increases. During obesity, the fat cells in the body increase in size due to the fat accumulation in the fatty cells. The increase in fat concentration causes insulin resistance in the obese person causing type II diabetes. Thus, in addition to many problems, obesity is a significant contributor to the development of diabetes, also known as diabesity. (9)

Cancer:
Obesity increases the risk of many cancers in the body, including cancer of the esophagus, breast, whole gut, gallbladder, kidney, liver, thyroid, brain, and ovaries.

The release of many growth factors by the fat cells in the obese person is responsible for developing the tumor cells in the body. Also, the obese person has more hormones like sex and insulin-like growth hormone. The factors released from the fat cells and the greater amount of hormones in the body increase cell turnover and predispose the body to a greater risk of developing tumors and malignancies. (2)
Figure 5 SHOWS THE ASSOCIATION BETWEEN OBESITY AND DIFFERENT KIND OF CANCERS
Atherosclerotic cardiovascular disease due to obesity (ASCVD)
In obesity, atherosclerotic cardiovascular disease follows by the main disposing factor called metabolic syndrome. In obesity, metabolic syndrome is the common feature that plots an area for the development of atherosclerotic cardiovascular disease (10). The metabolic syndrome is characterized by the
- Hypertension
- Increase waist circumference
- High triglycerides in the blood
- Low Blood HDL
- High fasting blood sugar
The metabolic syndrome associated with obesity increases the risk of atherosclerotic cardiovascular disease by two times.
What is atherosclerosis?
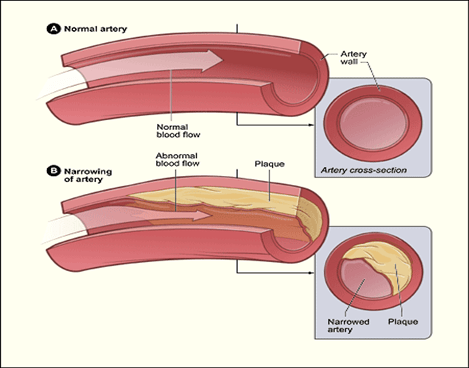
Atherosclerosis is the condition in which the cavity of the blood vessels decreases with the deposition of fatty substances in the vessels’ inner lining. This leads to the thickening and hardening of the vessels. These fatty substances include fatty acids, cholesterol, and the wastes of the cellular products mixed with calcium and coagulation factors like fibrin.
How does atherosclerosis affect the body?
Atherosclerosis affects the different arteries of the body, leading to the development of many cardiovascular system diseases(11)(12). The blood flow to the organ supplied by the atherosclerotic artery reduces, and the organ’s functioning is compromised. In severe cases, the artery blockage completely deprives the organs of the blood supply and leads to ischemia. The main organ affected by atherosclerosis is the heart. The heart is the body’s main organ supplying the whole body with blood. If the heart function is compromised, the entire body is affected
Change in fat composition of blood leading to fat deposition in the vessels
When someone suffers from obesity, the following change occur in the fat content of the blood
- Increased total TAG
- Increased very-low-density and low-density lipoproteins in the blood along with raised apolipoprotein B.
- Decreased high-density lipoproteins in the blood
The level of triglycerides-rich lipoproteins in the blood increases, which is the major contributor to the development of fatty depositions in the blood vessels. In a case-control study, researchers found that low-density lipoproteins are the main culprit in forming fat deposits within the vessels and increase the risk of cardiovascular disease by 3-times. So, we can say that the risk of fat deposit formation within the vessels is directly related to the elevated level of low-density lipoproteins(13).
Similarly, when the levels of the high-density lipoproteins in the blood decreases, the risk of forming fat deposits in the body increases. The low level of the high-density lipoproteins in the body increases apoprotein B, a precursor for these deposits in the vessels. As obesity reduces high-density lipoproteins, it indirectly acts as a risk factor for cardiovascular disease(14).
Increase in the blood coagulation factors
The production of several factors from fat cells in an obese individual disturbs the clot formation pathway. The fat cells produce the following factors;
- Plasminogen activator inhibitor-1 (PAI-1)
- Interleukin-6
- Tumor necrosis factor-a
All these products result in a hyperactive clot-forming mechanism in the blood by disturbing the inner surface of the blood vessels. Also, the levels of the procoagulant in the plasma of the obese person are higher compared to the non-obese person. The disruption of the clot formation process and the fibrinolytic abnormalities cause the formation of many thrombi in the blood vessels and enhance endothelial dysfunction. The leptins produced by the fatty tissue further disrupt the hemostasis and enhance endothelial dysfunction. This condition is the leading factor contributing to developing chronic conditions of the vessels that cause cardiovascular disease and other vascular abnormalities (14)(15).
Increase in the inflammatory mediators
A proinflammatory phase exists in an obese individual due to the release of C-reactive protein from the abnormally deposited fat in the body responsible for the fat deposit formation in the vessels. The continuous lipid-induced injury followed by the proliferation of the smooth muscles and the macrophages promotes the thickening of the blood vessels (16).
References
1-Kovesdy C, Furth S, Zoccali C, Li PKT, Garcia-Garcia G, Benghanem-Gharbi M, et al. Obesity and kidney disease: Hidden consequences of the epidemic. Indian Journal of Nephrology [Internet]. 2017 Mar 1 [cited 2022 Jul 2];27(2):85. Available from: /pmc/articles/PMC5358165/
2-Henley SJ, Thomas CC, Lewis DR, Ward EM, Islami F, Wu M, et al. Annual report to the nation on the status of cancer, part II: Progress toward Healthy People 2020 objectives for 4 common cancers. Cancer. 2020 May 15;126(10):2250–66.
3-Effect of Obesity on Your Bones and Joints | Ramsay Health UK [Internet]. [cited 2022 Jul 2]. Available from: https://www.ramsayhealth.co.uk/about/latest-news/effect-of-obesity-on-your-bones-and-joints
4-Gómez-Apo E, Mondragón-Maya A, Ferrari-Díaz M, Silva-Pereyra J. Structural Brain Changes Associated with Overweight and Obesity. J Obes [Internet]. 2021 [cited 2022 Jul 2];2021. Available from: https://pubmed.ncbi.nlm.nih.gov/34327017/
5-Ma Y, Ajnakina O, Steptoe A, Cadar D. Higher risk of dementia in English older individuals who are overweight or obese. International Journal of Epidemiology. 2020 Aug 1;49(4):1353–65.
6-Amen DG, Wu J, George N, Newberg A. Patterns of Regional Cerebral Blood Flow as a Function of Obesity in Adults. Journal of Alzheimer’s Disease. 2020;77(3):1331–7.
7-Fabbrini E, Sullivan S, Klein S. Obesity and Nonalcoholic Fatty Liver Disease: Biochemical, Metabolic and Clinical Implications. Hepatology [Internet]. 2010 Feb [cited 2022 Jul 2];51(2):679. Available from: /pmc/articles/PMC3575093/
8-Fabbrini E, Sullivan S, Klein S. Obesity and Nonalcoholic Fatty Liver Disease: Biochemical, Metabolic and Clinical Implications. Hepatology [Internet]. 2010 Feb [cited 2022 Jul 2];51(2):679. Available from: /pmc/articles/PMC3575093/
9-Diabesity: How Obesity Is Related to Diabetes – Cleveland Clinic [Internet]. [cited 2022 Jul 2]. Available from: https://health.clevelandclinic.org/diabesity-the-connection-between-obesity-and-diabetes/
10-Obesity and Metabolic Syndrome [Internet]. [cited 2022 Jul 2]. Available from: https://www.news-medical.net/health/Obesity-and-metabolic-syndrome.aspx
11-Atherosclerosis – What Is Atherosclerosis? | NHLBI, NIH [Internet]. [cited 2022 Jul 2]. Available from: https://www.nhlbi.nih.gov/health/atherosclerosis
12-Atherosclerosis | Johns Hopkins Medicine [Internet]. [cited 2022 Jul 2]. Available from: https://www.hopkinsmedicine.org/health/conditions-and-diseases/atherosclerosis
13-Krauss RM. Dense low density lipoproteins and coronary artery disease. The American Journal of Cardiology. 1995 Feb 23;75(6):53B-57B.
14-De Pergola G, Pannacciulli N. Coagulation and fibrinolysis abnormalities in obesity. Journal of Endocrinological Investigation 2002 25:10. 2014 Mar 11;25(10):899–904.
15-Widlansky ME, Gokce N, Keaney JF, Vita JA. The clinical implications of endothelial dysfunction. J Am Coll Cardiol. 2003 Oct 1;42(7):1149–60.
16-Visser M, Bouter LM, McQuillan GM, Wener MH, Harris TB. Elevated C-Reactive Protein Levels in Overweight and Obese Adults. JAMA. 1999 Dec 8;282(22):2131–5.