

Relationship of Cholesterol and your health
| The Cholesterol Paradox blog |
Although you must have heard of cholesterol, you might not know what it is. So, before diving deep into the detailed discussion, let us clarify some aspects of cholesterol to you. For example, what exactly is cholesterol? What are its types? Why is it necessary for our life, and from where can you get it?
Cholesterol is a fat-like waxy substance carried in your bloodstream throughout the body. Our body is capable of synthesizing cholesterol naturally. It can also be obtained from the food you eat. The liver produces the majority of the cholesterol your body needs. Foods made from animal sources contain cholesterol. Cholesterol is an important structural element which makes up roughly 30% of cellular membranes. It serves to preserve the fluidity and structural rigidity of the membranes. Furthermore, it is also a precursor for producing steroidal hormones, vitamin D and bile acids in the body. This article will cover all the types of cholesterol and its relation to heart diseases.
What is meant by good and bad cholesterol
Cholesterol and other fats circulate in your bloodstream on proteins called lipoproteins. The most commonly known lipoproteins that carry cholesterol throughout the body are low-density lipoproteins (LDL) and high-density lipoproteins (HDL). They are explained in the text below.
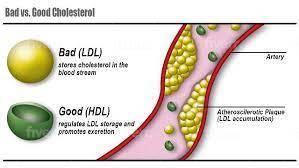
Low-density lipoproteins or bad cholesterol
Often described as LDL, low-density lipoproteins are referred to as bad cholesterol. This is because these are considered potential cause of heart disease. The optimum level of LDL safe for our body is less than 100 mg/dl. A level between 100-129 mg/dl is near or above normal. The level between 130-159 mg/dl is considered borderline high. You frequently hear about the need to lower cholesterol. This refers to lowering and maintaining LDL cholesterol. Because a high LDL level causes plaque to accumulate in your arteries, we will explain its phenomenon later.
High-density lipoproteins (HDL) or good cholesterol
High-density lipoproteins are also called ‘good cholesterol’ because it helps remove cholesterol from your arteries. HDL carries cholesterol from other parts of your body to the liver. The liver then eliminates this excessive cholesterol and protects your body from its harmful effects. Normal HDL levels are essential to protect you from heart disease. Your body’s desired level of HDL is 60 mg/dl. This level is considered to be protective against heart-associated complications (1). A level below 40 mg/dl in men and below 50 mg/dl in women is considered risky. Low HDL levels are a risk factor for heart disease in both men and women. So you must maintain your level to live a healthy life.
Very low-density lipoproteins (VLDL)
Often described as VLDL, very low-density lipoproteins carry triglycerides from all body parts instead of cholesterol and transport them to the liver for elimination. Triglycerides constitute the majority of the fat in your body. When you eat, your body converts excess calories into triglycerides which are then stored in fat cells. Later, hormones cause the release of triglycerides for energy between meals. If you eat more calories than your body requires, you may have high triglycerides. Hence, it is essential to have normal VLDL levels so that the excess triglycerides do not accumulate in your body. It isn’t easy to assess the VLDL. Triglycerides constitute almost half of VLDL. Hence you can calculate your VLDL level as a proportion of triglycerides.
How cholesterol and other lipids contribute to plaque formation and atherosclerosis?

You must know that low-density products usually float on the water’s surface. The same phenomenon applies to fats in our blood. As blood is thicker, it makes the process slow. The lipids do not disintegrate in blood, and those with low density start to leave the blood slowly and make deposits on the walls of capillaries by combining with other substances, which accumulate as part of an inflammatory reaction. These deposits gradually become larger, thus not only blocking blood flow but also causing blood vessels to narrow. The blood channels known as arteries transfer oxygen-rich blood from the heart to every organ in your body. The arteries become smaller due to lipid buildup on their inner surfaces. This accumulation of lipids on the inner side of arteries is called atherosclerosis. This narrowing of arteries leads to various complications. The most morbid among them is coronary artery disease.
Role of saturated fat in cholesterol production
Saturated fat is a type of dietary fat, but it is one of the unhealthy fats. Saturated fats are most often solid at room temperature. Your body requires healthy fats for energy and other functions. Excess saturated fat can cause cholesterol to accumulate in your arteries. They increase LDL cholesterol synthesis, which is known as bad cholesterol. Hence, they can lead to many health problems. So, it would be best if you tried to limit these in your diet. Saturated fats are mostly found in foods derived from animals, including cheese, meat, butter, and milk.
Cholesterol and coronary artery disease
The major factor for coronary artery disease is high cholesterol. Cholesterol accumulates in the walls of coronary arteries, ultimately causing localized constriction of vessels. This reduces blood flow to a section of the heart muscle supplied by constricted arteries. Furthermore, cholesterol plaques can separate and move into smaller arteries or capillaries, entirely or partially blocking the channel. Occasionally, inflammatory cells may also go to the site of fractured plaque, causing additional constriction. The decreased blood flow to the heart can lead to chest pain, also called angina. If the vessel becomes fully clogged, it can lead to a heart attack (2).
The global drive to reduce cholesterol through diet and medication has been unable to stop the global pandemic of coronary artery disease from spreading. It is explained below in the text.
Cholesterol hypothesis and the work of Ancel Keys
The cholesterol hypothesis states that cutting cholesterol content prevents cardiovascular disease. The work by Ancel Keys has also been based on the hypothesis that higher cholesterol levels are the major cause of heart disease. It was also referred to as the lipid hypothesis. The majority of the medical community agrees with the above concept due to a lot of evidence. At the same time, there are a lot of health professionals who argue about the validity of the concept. According to them, blood cholesterol level is not the only reason, and there is not sufficient evidence to prove the hypothesis of Ancel Keys. According to them, there are other factors which also contribute to heart diseases. This debate is termed the cholesterol paradox.
The Relationship between cholesterol and mortality has also been problematic, with several studies reporting an inverse association between cholesterol and mortality. The term cholesterol paradox was used when it was found that mortality remained high in patients with low cholesterol levels (3). This relation relates to the controversial concept of fats and heart disease. According to the disease control and prevention centres, it is also possible that persons with a family history of heart disease have shared settings that could raise their risk.
Cholesterol and heart disease
Although there is an agreed concept by the majority that the levels of cholesterol and the risk of heart disease are positively correlated, it is not always true. Recent studies have shown that cholesterol level may be one of the risk factors for heart disease but not the ultimate cause of it. Heart disease patients may not always have higher cholesterol than healthy people. Many other factors play a role in causing heart disease.
It would be best if you did not fear cholesterol as it is integral to our body structure. As explained above, it plays a role in membranes’ integrity and synthesizing hormones and bile acids. All these phenomena are crucial for our health and survival. But you should keep a check on your cholesterol levels. Eating a healthy diet and living a healthy lifestyle keep you away from many ailments. It is reasonable to assume that although cholesterol may influence health, health may also influence cholesterol.
Cholesterol-health Relationship
Cholesterol-health relationships may differ in subpopulations dependent on health status (7). While most of the time, it is thought that a higher cholesterol level in old age is a risk for many diseases. Recent studies have denied this concept. A study showed that increases in cholesterol over time have beneficial associations in some older adults (4). Another study showed that low cholesterol has also been associated with cancer risk. Population interventions to lower cholesterol could lead to an increased risk of cancer (5). Cell culture showed that cancerous cells secrete a factor that alters cholesterol metabolism (6).
Many factors can affect your cholesterol level. Smoking, alcohol intake, major and minor illnesses, hospitalization, heart attack, acquired immune deficiency syndrome (AIDS), weight change and selected medications are some factors that alter your cholesterol metabolism (8).
References
- Barter, P., Gotto, A. M., LaRosa, J. C., Maroni, J., Szarek, M., Grundy, S. M., Kastelein, J. J., Bittner, V., Fruchart, J. C., & Treating to New Targets Investigators (2007). HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events. The New England journal of medicine, 357(13), 1301–1310. https://doi.org/10.1056/NEJMoa064278
- Grundy S. M. (1986). Cholesterol and coronary heart disease. A new era. JAMA, 256(20), 2849–2858.
- Budzyński, J., Tojek, K., Wustrau, B., Czerniak, B., Winiarski, P., Korzycka-Wilińska, W., & Banaszkiewicz, Z. (2018). The “cholesterol paradox” among inpatients – retrospective analysis of medical documentation. Archives of medical sciences. Atherosclerotic diseases, 3, e46–e57. https://doi.org/10.5114/amsad.2018.74736
- Karlamangla, A. S., Singer, B. H., Reuben, D. B., & Seeman, T. E. (2004). Increases in serum non-high-density lipoprotein cholesterol may be beneficial in some high-functioning older adults: MacArthur studies of successful aging. Journal of the American Geriatrics Society, 52(4), 487–494. https://doi.org/10.1111/j.1532-5415.2004.52152.x
- Schatzkin, A., Hoover, R. N., Taylor, P. R., Ziegler, R. G., Carter, C. L., Larson, D. B., & Licitra, L. M. (1987). Serum cholesterol and cancer in the NHANES I epidemiologic followup study. National Health and Nutrition Examination Survey. Lancet (London, England), 2(8554), 298–301. https://doi.org/10.1016/s0140-6736(87)90890-7
- Ueyama, Y., Matsuzawa, Y., Yamashita, S., Funahashi, T., Sakai, N., Nakamura, T., Kubo, M., & Tarui, S. (1990). Hypocholesterolaemic factor from gallbladder cancer cells. Lancet (London, England), 336(8717), 707–709. https://doi.org/10.1016/0140-6736(90)92204-u
- Harris, T., Feldman, J. J., Kleinman, J. C., Ettinger, W. H., Jr, Makuc, D. M., & Schatzkin, A. G. (1992). The low cholesterol-mortality association in a national cohort. Journal of clinical epidemiology, 45(6), 595–601. https://doi.org/10.1016/0895-4356(92)90131-6
- Jacobs, D., Blackburn, H., Higgins, M., Reed, D., Iso, H., McMillan, G., Neaton, J., Nelson, J., Potter, J., & Rifkind, B. (1992). Report of the Conference on Low Blood Cholesterol: Mortality Associations. Circulation, 86(3), 1046–1060. https://doi.org/10.1161/01.cir.86.3.1046
- Glatz, J. F., & Katan, M. B. (1993). Dietary saturated fatty acids increase cholesterol synthesis and fecal steroid excretion in healthy men and women. European journal of clinical investigation, 23(10), 648–655. https://doi.org/10.1111/j.1365-2362.1993.tb00726.x